All Basics
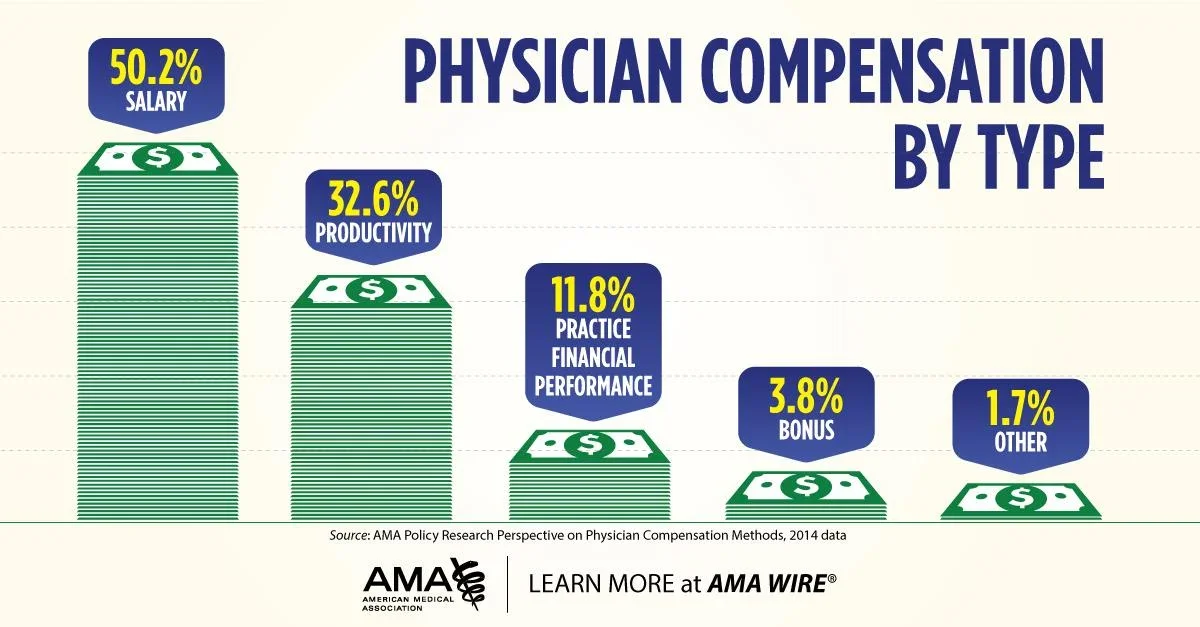
Physican Compensation: Remember, not all physicians have just a base salary, despite what we see at most job opportunities. Its important to ask what part of your “salary” has base vs productivity or RVU bonuses. We will discuss more about what RVUs mean shortly. Practice financial performance includes profit sharing from bonuses practices or hospitals receive from meeting quality metrics or participating in certain value-based care models. We will have a separate breakdown on value based care later, but beware if you participate in value-based care, depending on the type of contract and model, part of your salary may depend on “clinical outcomes” from metrics including # of colonoscopies completed, A1C <8, or even how many times your patient gets hospitalized for congestive heart failure.
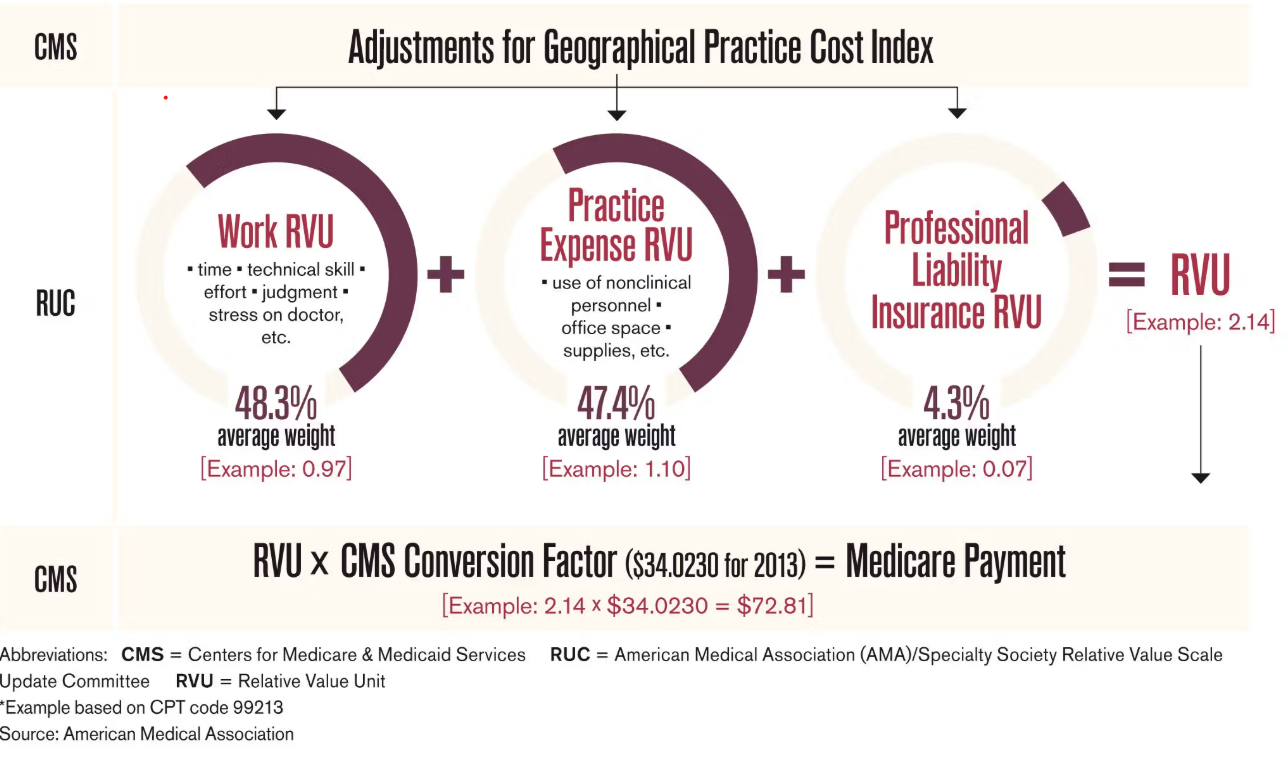
The RUC:
The RUC explains in more detail who sets the “Medicare Rate” establish above that influences payment even in the commercial space. It’s actually simple math! A committee of physicians recommends the “value” of surgery, procedure, and clinic visits/services with the number of RVUS (Relative Value Units) they assign. CMS (Commision of Medicare Services) applies a conversion factor (which as I showed has declined…) to set the “Medicare Payment” rate.
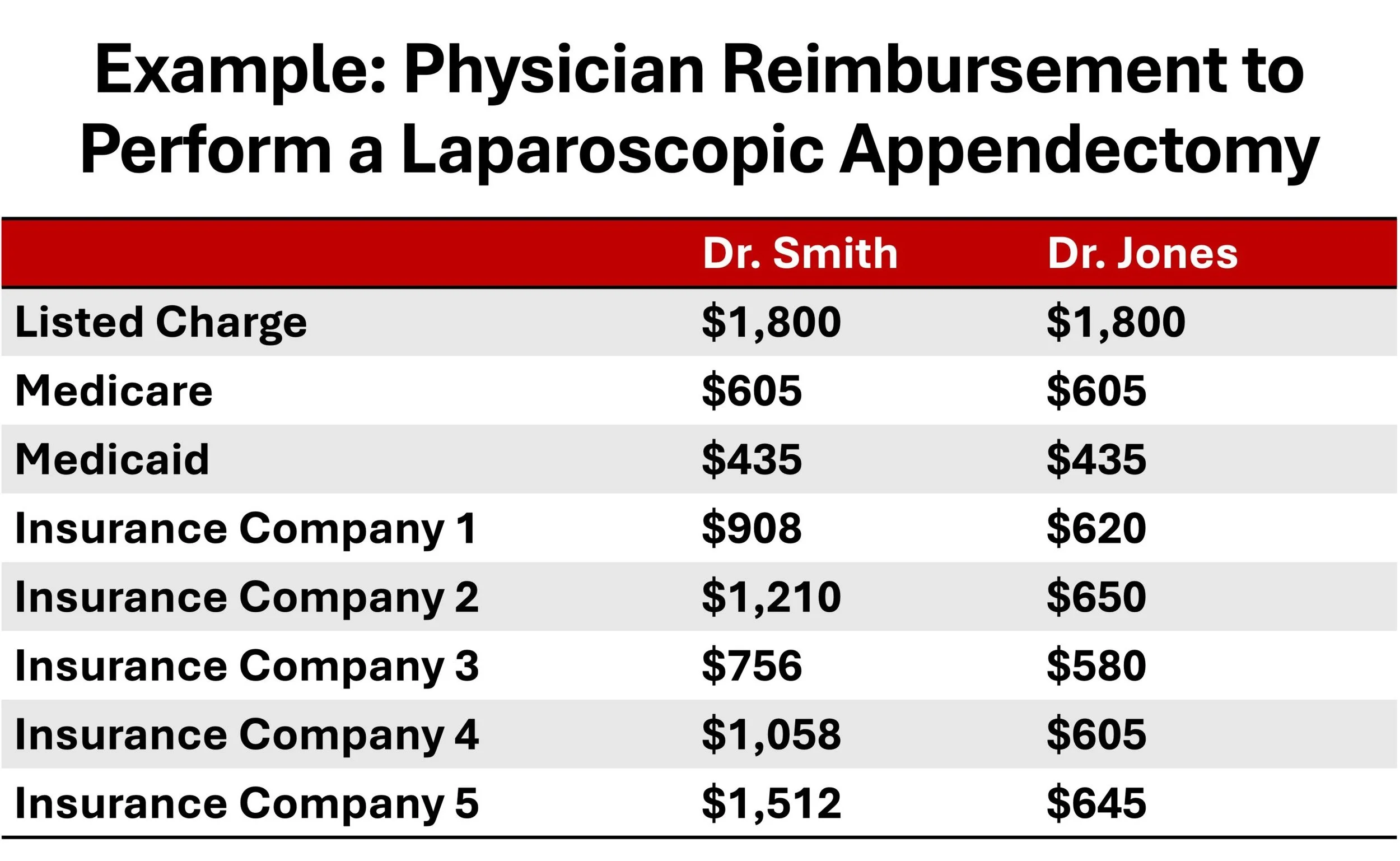
Your reimbursement depends on your “payor mix":
It totally shocked me in college to find out that our healthcare system pays physicians differently based on what time of insurance a patient has as well as how much that physician negotiates. The private industry uses the Medicare rate determined by the RUC and CMS as described above as a benchmark to typically pay X times the Medicare rate, and Medicaid typically pays a fraction X of the the Medicare Rate. Basically, Commercial/Private Insurance > Medicare > Medicaid in terms of payment.
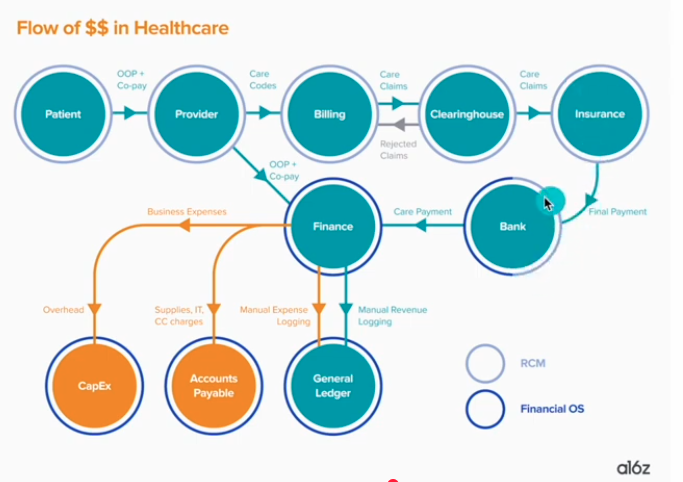
Basics of Revenue Cycle: I really just put this here because I love this diagram to show how the money moves! It basically summarizes what we call “revenue cycle management.” In healthcare, we spend approximately 10-15% of our money just hiring people to manage this whole process to reduce metrics such as “rejected claims” or “late payments.” Basically, it takes a lot of money to make sure we get our money!
Notes:
Both patients and physicians do not know how doctors actually make money. The lack of knowledge means patients do not trust their doctors when they should, and other times they do when they should not! It also means young doctors do not know how to make the best career decisions for themselves because no one ever talks about how their practice will actually work in the real world. It is why I started this series with this video on “How do doctors make money?”, because fixing the healthcare industry requires everyone to understand how the money flows. Yes, healthcare costs a ton, and no it’s not the individual doctor’s fault. We live in a system driven by money; but, the majority of healthcare costs comes from administration, insurance, drugs & devices — not your individual doctor’s salary.
Yes, depending on who employs the doctor and what kind of doctor they are, they are incentivized to “do” more to get more money. The hard truth? In medicine, there exists a lot of gray area on what is “medically indicated 100%” vs “could be medically indicated but also could not” vs “medically unnecessary but not harmful” vs “plain harmful.” Do 99% of physicians do harmful procedures or labs to gain more money? No. But, do physicians play “could or couldn’t be medically indicated, but not harmful” side if they can get more money? Of course they do. Do they make money from prescribing you a specific drug? No. Do they get lunches constantly from medical device and pharmaceutical representatives to encourage certain drugs and devices? Yes. No, we do NOT get money from recommending vaccines.
Resources: